When Your Body Won't Let Go: The Real Link Between Chronic Pain and Trauma
You've been to the doctors. You've done the scans. Maybe you've tried physio, massage, medication, or all three. And still — the pain persists. You're not imagining it. You're not weak. And you're definitely not alone.
What's often missing from these conversations is something that research has been quietly confirming for decades: chronic pain and trauma are deeply, biologically connected. Understanding that connection doesn't just explain why you hurt — it opens the door to a kind of healing that addresses the root, not just the symptom.
Pain Isn't Just Physical
Here's something that might surprise you: pain isn't produced in the body the way we often think. Pain is actually produced by the brain, as an output — a warning signal meant to protect you from harm. In the short term, this is incredibly useful. Touch a hot stove, feel pain, pull your hand away.
But when your nervous system has been shaped by trauma, those warning signals can get stuck. The alarm keeps ringing, even when there's no immediate danger. This is one of the central mechanisms behind chronic pain — and it's why treating the body alone often isn't enough.
A 2022 study published in Frontiers in Neuroscience described it this way: trauma-related symptoms are grounded in dysfunction at the level of the brainstem and spinal cord — the parts of the nervous system that govern how we process sensation, regulate arousal, and feel safe in our bodies. When those systems are dysregulated, pain signals get amplified and distorted.
The ACE Studies: How Trauma Gets Into the Body
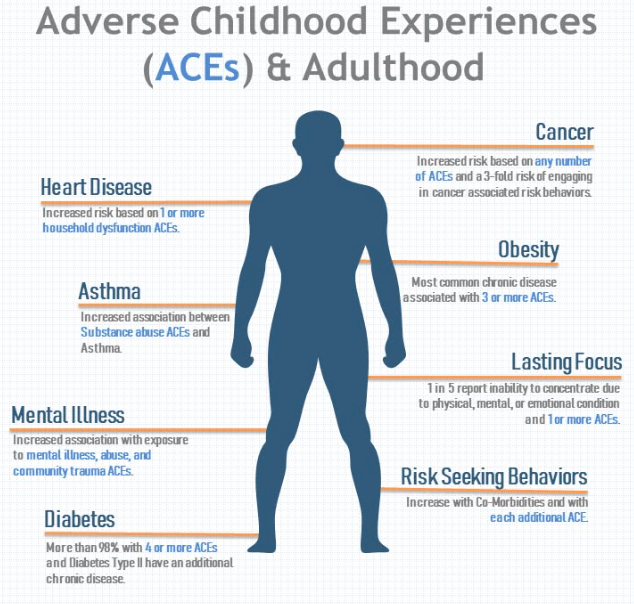
The most compelling evidence for the trauma-pain connection comes from the landmark Adverse Childhood Experiences (ACE) research — one of the largest studies ever conducted on the long-term health effects of childhood trauma.
The findings are stark: people who experienced abuse, neglect, or significant household dysfunction as children are dramatically more likely to develop chronic pain as adults.A 2023 meta-analysis pooling data from 57 studies found that people with at least one adverse childhood experience were 45% more likely to report chronic pain in adulthood. Those with four or more ACEs had significantly higher risk still.
"The presence of early trauma appears to confer a two- to three-fold risk of later development of chronic pain." — Jackson, W.C., Practical Pain Management (2020)
Source: Jackson W. Connecting the Dots: How Adverse Childhood Experiences Predispose to Chronic Pain. Pract Pain Manag. 2020;20(3).
Emotional abuse, in particular, showed some of the largest effect sizes in several major studies — meaning it's not just physical trauma that leaves a physical mark. Words, neglect, chronic fear, and relational insecurity all shape the nervous system, too.
The Spine, the Nervous System, and the Body That Remembers
You may have heard the phrase popularized by Dr. Bessel van der Kolk: "the body keeps the score." This isn't just a metaphor — it reflects real neurobiological mechanisms that researchers are continuing to map.
When the body experiences trauma, the stress response (governed by the hypothalamic-pituitary-adrenal, or HPA, axis) activates the familiar fight, flight, or freeze state. In the moment, this is adaptive — it keeps you alive. But when trauma is chronic, repeated, or unresolved, the HPA axis can become dysregulated. The body stays in a state of low-grade activation, flooding tissues with stress hormones, tightening muscles, and sensitizing pain receptors.
Crucially, this sensitization happens at the level of the spinal cord. A process called central sensitization means that nerve pathways in the spine literally become more reactive over time — lowering the threshold at which pain signals are sent to the brain. As ScienceDirect researchers describe it, persistent spinal cord stimulation leads to hypersensitivity at the affected segments, sensitizing related regions of the brain as well. Trauma can literally rewire the nerve pathways in your spine. Put simply: your body has been turned up too loud for too long — and it doesn't know how to turn itself back down without help.
This is why a seemingly minor touch, posture shift, or even emotional stress can trigger intense pain in someone with a trauma history. The spine and nervous system have been recalibrated toward hypervigilance — and pain is the result.
Here's something most people living with chronic back or spine pain have never been told: unresolved trauma and chronic stress don't just change how your nervous system processes pain — they may be changing the physical structures of your spine itself. Research has found that sustained high cortisol levels — the direct result of a nervous system stuck in survival mode — can impair the disc cells that keep your spine cushioned and resilient, compromising their ability to regenerate and repair. Over time, the chronic muscle tension that trauma survivors often carry creates abnormal mechanical load on discs, ligaments, and joints, accelerating the kind of wear the body would otherwise be able to manage. The trauma isn't just a memory. In very real, biological terms, it is living in your body — and it is worth treating as such.
It's also important to note that this isn't a sign of weakness or "it's all in your head." These are measurable physiological changes. The pain is absolutely real. It just has roots that standard pain management often doesn't reach.
PTSD and Chronic Pain: A Cycle That Feeds Itself
Chronic pain and PTSD don't just co-occur — they actively fuel each other. Research published in ScienceDirect (2025) describes what's called a "mutual maintenance model": PTSD and chronic pain reinforce one another through shared mechanisms like hypervigilance, avoidance, and negative emotional processing.
People with PTSD are also significantly more likely to experience severe and persistent pain. A 2025 systematic review found that between 10 and 26 percent of chronic pain patients meet full diagnostic criteria for PTSD — and many more carry subclinical trauma symptoms that still meaningfully affect their pain experience.
What's particularly striking is how emotional states create predictable patterns in the body. Anxiety keeps muscles braced — especially in the upper back, shoulders, and lower back. Depression changes how the brain processes pain signals, making the same stimulus feel more intense. Unresolved grief and shame can show up as tightness, heaviness, or a persistent ache that defies medical explanation.
None of this means the pain isn't real. It means the pain has a story — and that story matters for how we treat it.
How Therapy Can Help — Including EMDR
If chronic pain is, in part, a nervous system problem rooted in unprocessed trauma — and if that trauma has been quietly elevating stress hormones, impairing the body's ability to heal, and keeping muscles braced against a threat that never fully passed — then trauma therapy isn't just a mental health intervention. It's a physical one.
This is worth sitting with for a moment. When the nervous system finally feels safe:
Cortisol levels drop — and disc cells can regenerate more effectively
Chronic muscle bracing releases — reducing the mechanical load on spinal structures that has been accumulating for years
The inflammatory response settles — giving injuries that have resisted healing the internal conditions they finally need
Therapy doesn't just change how you experience your pain. It may change the biological environment in which your body is trying to recover.
EMDR: Treating the Alarm, Not Just the Smoke
One of the most researched approaches for this intersection is EMDR, or Eye Movement Desensitization and Reprocessing. Originally developed to treat PTSD, EMDR uses bilateral stimulation — typically guided eye movements — to help the brain reprocess traumatic memories in a way that reduces their emotional and physical charge.
The mechanism matters here. EMDR appears to separate the connections between traumatic memories and the physiological alarm response they trigger. Less alarm means less cortisol, less bracing, less inflammation — and research suggests, less pain.
EMDR has been shown in randomized controlled trials to significantly reduce pain intensity across a wide range of conditions:
Chronic musculoskeletal pain and back pain
Headaches and migraines
Fibromyalgia
Phantom limb pain
Rheumatoid arthritis
"Some people who have been almost completely non-functional due to pain can achieve very low levels and, at times, completely abated pain." — EMDR International Association
Crucially, follow-up studies show these improvements tend to hold. This isn't temporary relief — it reflects genuine, lasting change in how the nervous system is functioning.
Other Approaches Worth Knowing About
EMDR isn't the only tool. A growing body of trauma-informed therapies are showing real results for chronic pain:
Somatic Experiencing (SE) — developed by Dr. Peter Levine, SE works directly with held tension patterns in the body, helping the nervous system complete the responses that trauma interrupted. Researchers have described unresolved PTSD as a potential "missing link" in why some people's chronic low back pain persists despite standard treatment — and SE has been studied specifically for this combination.
Internal Family Systems (IFS) — works with the parts of us that have been carrying pain, fear, and protective responses, often for decades.
Trauma-informed CBT — addresses the thought patterns and avoidance behaviours that keep both PTSD and chronic pain locked in place.
Mindfulness-based interventions — build the capacity to be present with sensation without amplifying it, gradually retraining the nervous system's threat response.
It's important to be honest: therapy won't reverse severe structural damage or replace medical care. But for the many people whose pain has roots in trauma, stress, or a nervous system that never got to complete its recovery, addressing those roots can change everything.
Working With Dee Martin at The Relationship Agency
At The Relationship Agency, we believe that healing chronic pain often means working with the whole person — and that sometimes, the most important thing a body needs in order to heal is for the nervous system to finally feel safe.

Dee Martin, MSW, RSW
Dee Martin is one of our experienced clinicians working specifically at the intersection of trauma and the body. What Dee offers:
A trauma-informed lens that looks beyond the symptom to what the body may be holding
Experience working with clients whose pain hasn't responded to conventional treatment
A warm, grounded approach that moves at your pace — this work is never forced
Support for pain that has been labelled structural, stress-related, or simply unexplained
The transformation that's possible here goes beyond symptom management. Clients who come to this work often describe not just reduced pain, but a fundamentally different relationship with their bodies — one built on safety rather than bracing, on presence rather than protection. That shift, it turns out, isn't just psychological. It's biological.
You Deserve More Than Pain Management
There's a difference between managing pain and healing from it. Management keeps you functional. Healing gives you your life back.
If you've been living with chronic pain — especially pain that has roots in difficult experiences, high stress, or a history of trauma — therapy isn't a last resort. For many people, it's the thing that finally works.
You don't have to keep white-knuckling your way through it. Help is available, and transformation is possible.
→ Book a consultation with Dee Martin or another member of our team at The Relationship Agency.
References
Karimov-Zwienenberg M, et al. Childhood trauma, PTSD/CPTSD and chronic pain: A systematic review. PLoS ONE. 2024;19(8):e0309332.
Taylor & Francis Group. Childhood trauma increases risk of chronic pain in adulthood. ScienceDaily. December 2023.
Jackson W. Connecting the Dots: How Adverse Childhood Experiences Predispose to Chronic Pain. Pract Pain Manag. 2020;20(3).
Critchley HD, et al. Emotional and autonomic consequences of spinal cord injury. Brain. 2006;129(3):718–728.
Kozlowska K, et al. The brain-body disconnect: A somatic sensory basis for trauma-related disorders. Frontiers in Neuroscience. 2022.
Tesarz J, et al. EMDR Therapy's Efficacy in the Treatment of Pain. Journal of EMDR Practice and Research. 2019;13(4).
Frontiers in Psychology. Group EMDR in chronic pain patients. 2024.
Vock S, Tesarz J. EMDR in pain therapy. PubMed. 2025.
EMDR International Association. EMDR Therapy and Chronic Pain. 2024.
BMC Complementary Medicine and Therapies. Somatic Experiencing for patients with low back pain and PTSD. 2018.
ScienceDirect. PTSD and chronic pain: A systematic review and meta-analysis. 2025.